 New
New Behaviour Management and BPSD
CPDTime.
12m
Published: 24 May 2023


Published: 24 May 2023
Challenging behaviours are a common symptom of many conditions, such as intellectual disability, autism and dementia.
When poorly managed, these behaviours can have far-reaching effects, including distress for the client, disruptions to the lives and comfort of other clients, and added stress and workloads for healthcare workers.
In a home or aged care setting, the behavioural and psychological symptoms of dementia (or BPSD) are common, however, still remain one of the biggest challenges to care staff. One study found that while many residential aged care staff understood the underlying causes of BPSD, they lacked the appropriate management skills and resources to deal with them appropriately (Ervin et al. 2012).
Mishandling of BPSD can lead to the inappropriate use of restrictive practices, which should be a last resort for care staff, but have time and time again been incorrectly used as a frontline approach to changed behaviours.
Appropriate behavioural management is not only essential to maintaining a high quality of life and comfort for all clients, but it is also directly tied to Standard 1: Consumer Dignity and Choice, Standard 7: Human Resources and Standard 8: Organisational Governance of the Aged Care Quality Standards.
The following tips will provide carers with a foundational understanding of behaviour management to ensure their clients receive effective person-centred care when displaying BPSD.
There are countless ways to handle changed behaviours, however, approaching the situation methodically with an assessment tool like the ABC Approach to Behaviour Management examines the behaviour from a person-centred perspective. The aim of this type of approach is to help us understand the aetiology of the behaviour and develop a suitable, consistent response for ongoing support (Crombie et al. 2007; Autism Spectrum Australia 2014; Krishnamoorthy & Anderson 2011).
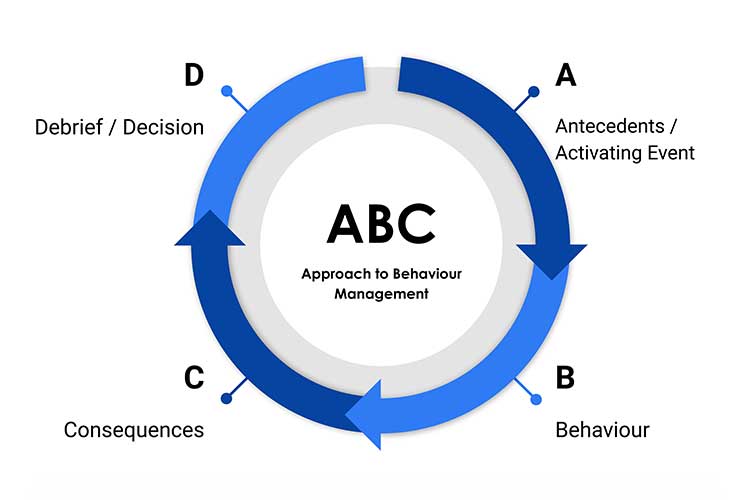
(Loddon Mallee Regional Dementia Management Strategy n.d.)
The antecedent or activating event looks at direct or indirect triggers of the behaviour; the why, what, when, where and who.
These stimuli could include:
(ABIOS 2021)
The changed behaviour should be defined clearly. Types of BPSD commonly seen include:
(Tible et al. 2017; Health.vic 2015)
Note, simply labelling the behaviour is not sufficient. You must be able to describe what was observed. For example, did the client yell, cry, punch or use particular words?
The consequences of the behaviour are the responses from everyone involved. These could include those of the staff, family members or other residents who were witness to the behaviours.
(Synapse 2021)
The final and additional step to the ABC Approach is to decide and debrief. This step allows the care team to come together to consider their findings and collaborate on the best way to manage the situation. Remember that in true client-directed care, the client themself is part of the care team and should be involved in this process, or alternatively, the client’s family or designated decision-makers.
Decisions on what actions to take could involve:
(Alzheimer’s Society 2021; Health.vic 2015)
Scenario: Ted is an 87-year-old resident in a secure aged care facility who is living with dementia. In his younger years, Ted was extremely active and would wake early every morning to walk to the corner milk bar to buy the newspaper.
Antecedent or Activating Event: |
After waking early one morning, Ted attempts to leave through the front entrance of the facility, with the intention of walking to the shop to buy the newspaper. However, he is halted by the locked security-door, which requires a keycode to open. |
Behaviour: |
Ted gets agitated and upset finding himself locked behind the door and begins to try to rattle and break the door latch. He is panicked and loudly demanding to be let out. |
Consequences: |
The staff member on shift responds to the behaviour in a confrontational manner (‘Hey! Stop that! What are you doing?! You’ll break the door! Go back to bed!’), attempting to stop Ted from waking and disturbing other residents. The staff member forcefully grabs hold of Ted’s wrists in an attempt to stop him from breaking the door lock. The staff member’s response only makes Ted more upset, increasing his distress. His behaviour continues to escalate into yelling and physical aggression. |
Decide and Debrief: |
After the incident, the care team debriefs with Ted’s family and learn about his history, habits and preferences of walking to get the newspaper each morning. The team also notes that the response of the staff member who was on shift was inappropriate and recommends they take a day away from work to de-stress and undergo further communication and de-escalation education. The team decides that the staff member rostered on each morning should now have a newspaper ready to offer Ted when he gets up in the morning, and respectfully offer to walk with him around the facility before returning him back to his room. |
The ABC Approach to behavioural management works best when the client’s behaviour is clearly documented and understood. The first approach should always be non-pharmacological and should involve tweaking the personal and environmental elements that contributed to the event.
The client’s medical prescriber may consider a medication review if the behaviours remain ongoing. Many milder behaviours tend to run a course and can resolve in time, and so patience and support is often the best response in these cases (Krishnamoorthy & Anderson 2011).
Note: Always refer to your facility's policy on dealing with difficult or aggressive behaviours. If there is a real risk of danger to you or your clients, security may need to be called.
Question 1 of 4
Step ‘C’ in the ABC Approach to Behaviour Management refers to…?


Ausmed Education is a Trusted Information Partner of Healthdirect Australia. Verify here.