This is usually the first and most important question parents ask after delivery. Answering that question accurately requires careful observation, thorough examination and, if needed, onwards referral for further assessment.
The aim of both the initial examination at birth and the full neonatal examination is to confirm normality, identify any congenital abnormalities and exclude medical concerns. It also gives the midwife a precious opportunity for further health education and parental reassurance (RCM 2012).
Initial Post-Delivery Assessment and Examination and APGAR Score
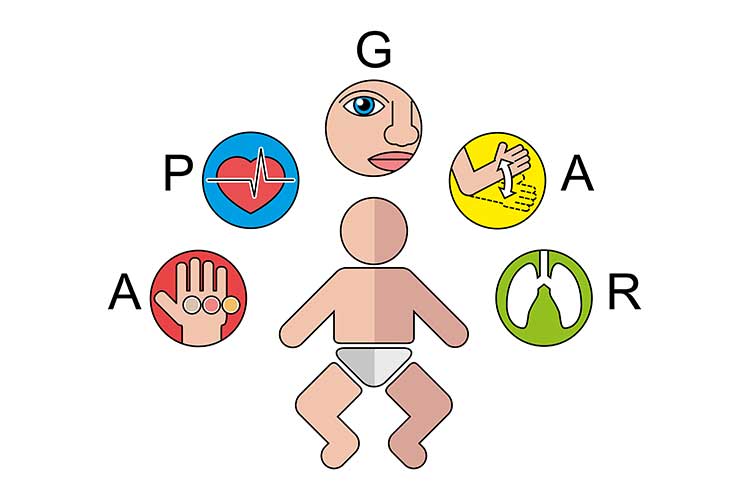
Monitoring successful transition to extra-uterine life begins from the moment of birth with an assessment of the APGAR score. This is measured at 1, 5, and if needed, 10 minutes after birth, and is followed by an initial examination soon after birth.
Score of 0
Score of 1
Score of 2
Appearance
Skin color
Blue or pale all over
Blue at extremities
Body pink
Acrocyanosis
No cyanosis
Body and extremities pink
Pulse
Pulse rate
Absent
< 100 beats per minute
> 100 beats per minute
Grimace
Reflex irritability grimace
No response to stimulation
Grimace on suction or aggressive stimulation
Cry on stimulation
Activity
Activity
None
Some flexion
Flexed arms and legs that resist extension
Respiration
Respiratory effort
Absent
Weak, irregular, gasping
Strong, robust cry
The initial post-delivery assessment aims to exclude obvious abnormalities and includes:
Assessment of colour to exclude pallor or cyanosis
Muscle tone, posture and responsiveness
Heart and respiratory rate
Normality of facial features, including eyes and mouth
Normal alignment spine and exclusion of spina bifida
Genitalia to exclude ambiguity
Trunk and limbs to exclude obvious abnormality
Assessment of the anus for patency
Evidence of birth trauma such as bruises or scalpel marks.
Birthweight, head circumference, temperature and the number of cord vessels are also recorded at this stage, and any concerns or abnormalities are reported to the paediatrician.
Full Newborn Assessment
This should generally be performed within 48 hours of birth, prior to discharge (Queensland Health 2019).
The aim of this more thorough examination is to:
Identify acutely unwell newborns who require urgent treatment
Review and address the family’s concerns about the newborn
Review suspected or identified issues related to antenatal screening, family history or labour
Review the newborn’s weight and head circumference
Assess whether urine and meconium have been passed
Diagnose any congenital malformations and arrange any required management
Discuss matters relevant to the newborn (e.g. newborn care, feeding, Vitamin K, Hepatitis B and Bacille Calmette-Guerin (BCG) vaccines, reducing the risk of Sudden Unexpected Death in Infancy (SUDI))
Explain issues such as jaundice that may arise in the following days or weeks
Discuss local networks, services and access to primary healthcare
Discuss how the family is able to access additional support if required.
(Queensland Health 2019)
Newborn Screening
Newborn screening involves a heel prick test that is performed 48 to 72 hours after birth. It is used to screen for 25 rare conditions, including:
Gathering Relevant Information Prior to Examination
Anticipated problems based on the maternal and family history
Factors affecting wellbeing during pregnancy and birth such as poor fetal growth
Date, time, type of delivery and birth weight
Whether the baby has passed urine and meconium.
Prior to the examination, maternal consent should be obtained, the procedure should be explained, and where possible, the examination should take place at the bedside with the mother present. Including the mother (or both parents if possible) gives the midwife a valuable opportunity to observe the parent’s interaction with their baby and address any general concerns they may have.
The Newborn Examination:
Observe the baby’s general condition, including colour, responsiveness, activity, spontaneous movement, posture and muscle tone. This should be assessed while the newborn is quiet, alert and not hungry or crying.
Assess the head and skull. Note facial symmetry, fontanelles, sutures, any scalp lacerations or lesions and the presence of any remaining caput, cephalhaematoma or trauma.
Examine the eyes for size, structure, position and red-eye reflex. Indications for further investigation include a hazy cornea, absent red eye reflex, conjunctivitis, yellow sclera or pupils that are uneven, dilated or constricted.
Note the position, structure and cartilage of the newborn’s ears. Unresponsiveness to noise, ear drainage or an absent external auditory canal or microtia are indications for further investigation.
Assess the mouth and palate for size, symmetry, movement, shape and structure. Inspect for craniofacial abnormalities such as a cleft lip or mouth drooping.
Assess the position and symmetry of the nose (nares and septum).
Assess the neck for structure, symmetry, range of movement, the thyroid and other masses.
Check the limbs, hands, feet and digits, assessing proportions, length, structure and symmetry. Examine feet to exclude any postural abnormalities such as talipes.
Assess the cardiovascular system. Khalilian et. al. (2016) reports that auscultation is one of the most important procedures in routine examination of neonates to identify congenital heart disease (CHD). Yet, differentiating between innocent and pathologic murmurs during auscultation is very hard and usually unfeasible. Check the newborn’s pulses, perfusion, heart rate, heart rhythm, heart sounds and pulse oximetry.
Check the lungs. Observe the rate and pattern of chest movement. Listen to the air entry to check for crackles and stridor. Note the presence of any respiratory problems such as tachypnoea at rest, retraction, grunting, or nasal flaring.
Observe the newborn’s abdomen for shape, symmetry and tenderness. Gently palpate to identify any organomegaly, masses or hernia. Confirm the presence of bowel sounds. The condition of the umbilical cord should also be noted.
Observe the newborn’s genitalia and anus to check for normal appearance, positioning and patency. Check whether the newborn has passed urine and meconium.
Palpate testes in male infants for presence or an undescended position. Cryptorchidism (failure of one or both of the testes to descend into the scrotum) affects approximately 2-6% of male babies born at term and is associated with a significant increase in the risk of testicular cancer and reduced fertility. Bilateral undescended testes may also be associated with ambiguous genitalia or an underlying endocrine disorder. According to Public Health England (2016), early diagnosis and intervention improves fertility, reduces the risk of torsion and may aid earlier identification of testicular cancer.
Examine the back. Inspect the bony structures and skin of the baby’s spine, with the baby prone. Note the presence of dimples, hair tufts, naevus, or abnormal skin patches.
Note the colour and texture of the skin as well as the presence of any birthmarks, rashes, swelling or abrasions.
Assess the reflexes and central nervous system. Observe tone, behaviour, movements and posture. The grasp, moro and sucking reflexes are assessed.
Check the hips, symmetry of the limbs and skin folds. Perform Barlow and Ortolani’s tests to exclude dislocation.
(Queensland Health 2019)
Routine Follow-Up
Parents should be informed that follow-up examinations will be performed at five to seven days of age and again at six weeks of age (Queensland Health 2019).
 New
New