Hypothermia: Reversible Causes of Cardiac Arrest Series
CPDTime.
3m
Updated 07 Aug 2020
This article is part of a series outlining reversible causes of cardiac arrest.
What is Hypothermia?
Hypothermia occurs when the core body temperature drops to below 35°C (95°F) (Mayo Clinic 2020).
The term primary hypothermia is used when the ability of an otherwise healthy person to maintain their core body temperature is overwhelmed by excessive cold temperatures, particularly when energy stores within the body have been depleted (Davis 2018).
Secondary hypothermia is when hypothermia is associated with acute events or illness, such as cerebrovascular accident (CVA), diabetic ketoacidosis (DKA) or burns. Secondary hypothermia can occur even where the environment is warm (Duong & Patel 2020; Davis 2018).
When the body is exposed to the cold, the initial response is to increase active movement and start shivering. Consciousness, breathing, and circulation initially remain intact but become increasingly impaired as the body cools more and more. If the core temperature falls to less than 32°C (90°F), atrial fibrillation is common, but this is not a significant cause for concern unless there are other indicators of cardiac instability (Brown et al. 2012).
Hypothermia Treatment and Management
If hypothermia is suspected, it is important to ascertain the patient’s core temperature. When infrared cutaneous, aural, or oral thermometers are used to measure temperature in patients with hypothermia, the results are often inaccurate. Measurement of the core temperature requires a properly calibrated, low-reading thermometer, but the accuracy of the reading may still vary depending on the site used, perfusion, and the temperature of the environment (Brown et al. 2012).
If a patient is intubated, the preferred method is a thermistor probe inserted into the lower third of the oesophagus to avoid false elevations as a result of ventilation with warmed gases. Alternatively, the thermistor probe can be placed into contact with the tympanic membrane; this will accurately reflect the brain temperature provided that the ear canal is clean and free of debris (e.g. cerumen) (Brown et al. 2012).
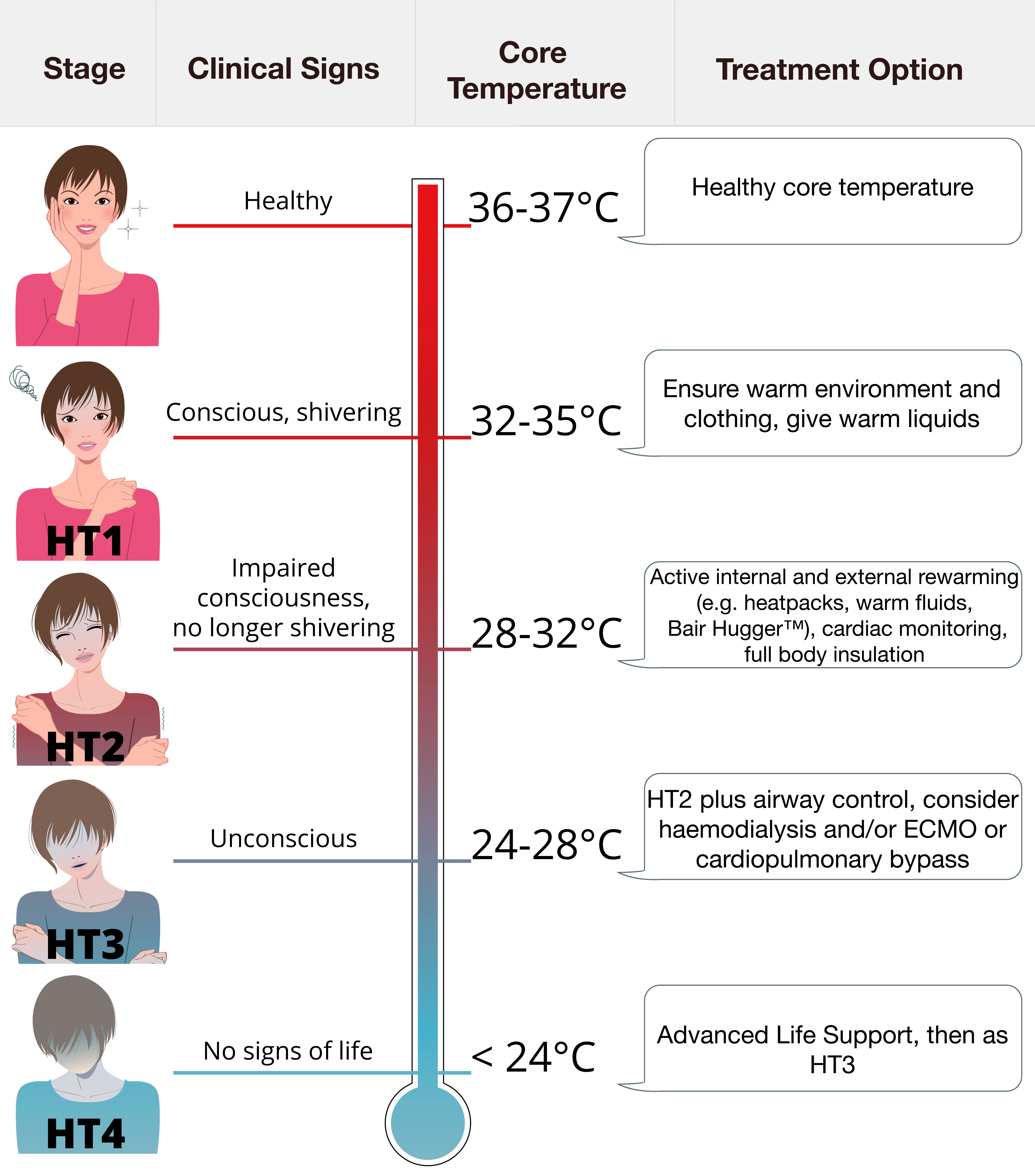
Swiss Staging System
If core temperature cannot be measured, the Swiss Staging System can be used to stage hypothermia based on presentation.
(Brown et al. 2012; Symons 2015)
Identifying and Managing Hypothermia During a Cardiac Arrest
The risk of cardiac arrest increases as the core temperature drops below 32°C, and increases substantially if the temperature reaches less than 28°C (Brown et al. 2012). At this level, a severe depression of critical body functions occurs, which may make the victim seem clinically dead during the initial assessment. It is vital, therefore, that lifesaving procedures are commenced unless death has undoubtedly occurred (i.e. presence of rigor mortis, decomposition, or injuries incompatible with life such as hemisection or decapitation) (Vanden Hoek et al. 2010).
Patients with hypothermia are often bradycardic (Soar et al. 2015) and may present in asystole (Vanden Hoek et al. 2010). Remember that detecting a pulse in a patient with hypothermia may be difficult, so signs of life and pulse should be checked carefully for a full 60 seconds. If no signs of life are detected, then cardiopulmonary resuscitation (CPR) should be started.
If return of spontaneous circulation occurs with basic life support (BLS) or advanced life support (ALS), full-body insulation and rewarming should be provided. This can commence during resuscitation as long as it does not impede CPR or delay transport (Brown et al. 2012).
Advanced airway management should be performed if indicated. Warm, humidified oxygen can be applied (Vanden Hoek et al. 2010). Intravenous (or intraosseous) fluids should be warmed to between 38 to 42°C to prevent further heat loss. In a cold environment, intravenous fluids will cool rapidly and may increase hypothermia. Large volumes of fluid are often required (Brown et al. 2012).
Choice of fluid is important. Normal saline can aggravate acidosis when given in large volumes, so crystalloids are often preferred. Vasopressors, such as adrenaline, may be used to treat hypotension due to vasodilation. These should be used with caution, however, because of the risk of complications such as cardiac arrhythmia and peripheral hypoperfusion - particularly significant in patients who are at risk for frostbite (Brown et al. 2012).
Look also at electrolytes – for example, a low serum potassium (hypokalaemia) may be a possible indicator of hypothermia as the primary cause of the arrest (Vanden Hoek et al. 2010).
There are many case reports indicating that survival from accidental hypothermia occurs, even with prolonged CPR and downtimes. From this comes the often heard, "nobody is dead until they are warm and dead" – essentially meaning that patients should not be considered dead before warming has been provided (Vanden Hoek et al. 2010).
Take-Home Message
Even in non-monitored settings, cardiac arrest is rarely a sudden, unpredictable event, as most patients demonstrate slow but progressive physiological deterioration. Hypothermia is an unusual aetiology for cardiac arrest, particularly in acute inpatient settings, but must not be excluded from consideration as a potentially-reversible cause. As with other causes, if it is unnoticed or poorly managed, poorer outcomes result.
Early, effective recognition and response to signs of hypothermia may prevent some cardiac arrests, deaths and unanticipated ICU admissions (Soar et al. 2015).
Australian Resuscitation Council & New Zealand Resuscitation Council 2018, ANZCOR Guideline 11.2 – Protocols for Adult Advanced Life Support, ANZCOR, East Melbourne, VIC, Australia, Wellington, New Zealand, viewed 27 May 2016, https://resus.org.au/guidelines/
Brown, DJA, Brugger, H, Boyd, J & Paal, P 2012, ‘Accidental Hypothermia’, The New England Journal of Medicine, vol. 367, pp. 1930-38, viewed 2 August 2016, https://www.nejm.org/doi/full/10.1056/nejmra1114208
Vanden Hoek, TL, Morrison, LJ, Shuster, M, Donnino, M, Sinz, E, Lavonas, EJ, Jeejeebhoy, FM & Gabrielli, A 2010, ‘Part 12: Cardiac Arrest in Special Situations, 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care’, Circulation, vol. 122, no. 18, suppl. 3, viewed 2 August 2016, https://www.ahajournals.org/doi/full/10.1161/circulationaha.110.971069
Topics
For Teams
Assign to your staff
Assign mandatory training and keep all your records in-one-place.
 New
New