Compartment syndrome is an extremely painful condition that if presenting acutely is a medical emergency. Left untreated, it can result in serious consequences such as ischaemia, necrosis, amputation of the affected limb or even death (Torlincasi et al. 2022; Cleveland Clinic 2021).
Note: This Article will focus on the acute form of compartment syndrome.
What is Compartment Syndrome?
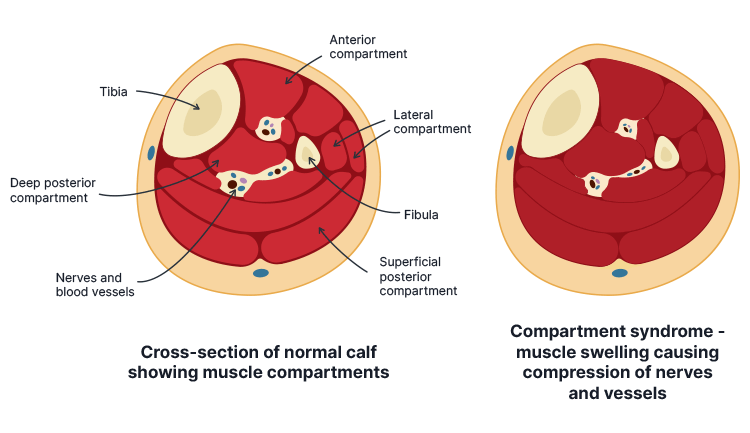
The arms and legs are divided into several segments known as fascial compartments. Each compartment comprises a group of muscle tissue, blood vessels and nerves contained within a strong membrane known as the fascia (Delgado & Morrison 2018).
The fascia is inelastic, preventing the compartments from rapidly expanding. Compartment syndrome is when blood or fluid accumulates in the intracompartmental space and the compartment is unable to stretch to accommodate this increased fluid volume, causing a high level of pressure, which in turn, impedes perfusion to the affected area (Torlincasi et al. 2022; ACI 2018).
Compartment syndrome most commonly occurs in the anterior compartment of the leg, but can also affect the forearm, thigh, buttock, shoulder, hand or foot (Physiopedia 2015).
There are two types of compartment syndrome: acute and chronic.
Acute compartment syndrome is typically associated with trauma and has a sudden onset. It’s a medical emergency that can result in significant disability or even death.
Chronic compartment syndrome is usually less serious and develops gradually, during or after intense physical exertion (e.g. exercise).
(Cleveland Clinic 2021; NHS 2019)
What Causes Acute Compartment Syndrome?
Potential causes of acute compartment syndrome include:
Bone fracture (most commonly a tibial shaft fracture)
Surgery (e.g. orthopaedic, nerve or vascular procedure)
(Hammerberg 2022; Healthdirect 2020; ACI 2018; Torlincasi et al. 2022)
Rarely, acute compartment syndrome can present without any signs of injury (NHS 2019).
Risk Factors for Acute Compartment Syndrome
Those at increased risk of compartment syndrome include:
Males under the age of 35 (possibly due to having a larger relative intracompartmental muscle mass and being at greater risk of sustaining a traumatic injury)
Children with paediatric leukaemia (some children with this condition have experienced acute compartment syndrome without sustaining any trauma)
People at increased risk of bleeding, including those:
Taking anticoagulants
With a family history of major bleeding
With a low platelet count
With severe liver or kidney disease.
(Torlincasi et al. 2022; ACI 2018)
Symptoms of Acute Compartment Syndrome
The onset of symptoms is typically within a few hours after sustaining trauma, however, in some cases, symptoms can develop up to 48 hours later (Torlincasi et al. 2022).
A patient with compartment syndrome may present with:
A tense, wood-like feeling in the affected compartment
Severe pain disproportionate to the injury (may be described as a burning sensation or a deep ache), which is exacerbated by passive stretching of the affected area and cannot be alleviated with analgesia
Paraesthesia
Pallor caused by vascular insufficiency (uncommon symptom)
Muscle weakness
Reduced sensation in the affected area
Paralysis (typically a later symptom).
(Torlincasi et al. 2022; TeachMe Surgery 2022; Hammerberg 2022)
Diagnosing Acute Compartment Syndrome
Compartment syndrome is typically identified via clinical diagnosis based on symptoms and risk factors, as prompt treatment is crucial (Torlincasi et al. 2022; TeachMe Surgery 2022).
Physical examination should involve:
Assessing the skin for lesions, swelling or discolouration
Palpating the compartment to assess temperature, tension and tenderness
Checking the patient’s pulse
A two-point discrimination test, which is used to assess whether the patient can identify that two objects touching the skin close together are separate objects rather than one
Assessing motor function.
(Torlincasi et al. 2022; Physiopedia 2021)
Traditionally, compartment syndrome has been diagnosed using the 'six Ps’ of arterial insufficiency:
Pain
Pulselessness
Paraesthesia
Paralysis
Pallor
Poikilothermia.
(Ovalle Jr & Megee 2019)
The six Ps are now considered clinically unreliable as aside from pain, they may only occur in the later stages of compartment syndrome by the time irreversible tissue damage has already occurred (Rasul Jr 2020; Hammerberg 2022).
The most reliable diagnostic method for compartment syndrome is measuring the intracompartmental pressure (ICP) of the affected area using a manometer or slit catheter. While this is not a necessary test, it can assist in confirming a diagnosis if uncertainty exists (Torlincasi et al. 2022; TeachMe Surgery 2022).
An ICP of over 30 mmHg indicates compartment syndrome (normal pressure is between 0 mmHg and 8 mmHg) (Torlincasi et al. 2022).
Other diagnostic tests that might be used include:
Radiograph if the patient has a suspected fracture
Doppler ultrasound to assess for occlusion or thrombus
Creatine kinase (CK) blood test (elevated CK levels are indicative of compartment syndrome)
Complete blood count and coagulation studies (preoperatively).
(Torlincasi et al. 2022; TeachMe Surgery 2022)
Note: Due to the severity of the condition and the potential for limb loss, treatment should be prioritised with less time spent on confirming the diagnosis (Torlincasi et al. 2022).
Once compartment syndrome is suspected, management steps might include:
Ensuring the affected limb is at a neutral level (not elevated or lowered)
Administering supplemental oxygen
Removing restrictive casts, dressings, or bandages from the affected limb
Preventing hypotension ad administering blood pressure support if necessary
Administering analgesia intravenously.
(Torlincasi et al. 2022; TeachMe Surgery 2022)
Compartment syndrome is treated using a surgical procedure known as a fasciotomy, wherein the skin is cut down to the fascia to release the accumulated pressure. The incision is then left open for several days to prevent the intracompartmental pressure from increasing again before being closed (ACI 2018).
Whether or not a fasciotomy is indicated generally depends on the ICP in the affected compartment and the amount of time that has elapsed since the trauma occurred, as if the injury is left untreated for too long, irreversible damage may have already ocurred (Torlincasi et al. 2022).
If necrosis has already occurred before a fasciotomy can be performed, an infection may be present. This may require debridement or even amputation to prevent systemic spread (Torlincasi et al. 2022).
The sooner a fasciotomy is performed, the more likely the patient is to recover their limb function. If left untreated for too long, the patient may experience residual nerve damage (Torlincasi et al. 2022).
Postoperative Care
Postoperative care might involve:
Physical therapy to help the patient restore function and strength in the affected limb, as well as prevent contractures and stiffness
Wound care and monitoring
An antibiotic regimen, if an infection is present
Analgesia
Use of an ambulatory device (e.g. crutches) while the injury is healing
Occupational therapy.
(Torlincasi et al. 2022)
Complications of Compartment Syndrome
Potential complications of compartment syndrome and fasciotomy include:
Cosmetic defects in the affected area
Recurrent compartment syndrome due to scarring
Pain
Contractures
Rhabdomyolysis
Nerve damage, which may lead to numbness and/or weakness
Infection
Acute renal failure
Death (usually occurs due to infection that leads to sepsis and multiorgan failure).
 New
New